
|
Articles Article 1 The Unwanted Child by Aaron Lederer, NCPsyA Abstract Disorders originating in the first two to three years of life stem from deficiencies in the infant contact with the primary provider, usually the mother. Clients who carry these early deficits cannot have rewarding, close relationships. They believe they are unwanted and fundamentally unlovable. Early in their lives, many of them made certain internal structural adjustments to best survive in their deficient environments. These adjustments and their consequences are identified and explained, and transactional analysis treatment to obtain the necessary restructuring is outlined. To have hate where there once was love, to have fear where there once was trust. -- A client This paper considers transactional analysis treatment for disorders originating in infancy. Berne (1961) defined the function of transactional analysis as helping clients put their Adult, uncontaminated, in the executive to obtain symptomatic control and relief. He asserted that transactional analysis is an advance over psychoanalysis for obtaining these results, but that additional work is required to obtain a cure. He maintained that cure, or deconfusion of the Child, is to be accomplished through script analysis, which is the substance of psychoanalysis. He called the process “psychoanalytic cure” (p.172); however, when it comes to clients with problems originating in infancy, Fried (1913/1958) concluded that they do not respond to psychoanalysis, and the analyst who undertakes to treat such a case “cannot fulfill his promise of cure” (p. 124). Whereas Freud's work emphasized the Oedipal conflict as the origin of neurosis, later writers (Klein, 1945/1975; Rinsely, 1989) recognized that more clients suffer from distress originating from earlier experiences. Little (19900) observed:
Such changes have indeed been taking place in the psychoanalytic field with advances such as ego psychology, object relations, self psychology, and Spotnitz's (1993) modern psychoanalysis, although success using these developments usually requires many years of treatment. Many transactional analysts have developed treatments for child-development problems: early work with permission workshops (Steiner, 1974); reparenting regressive work (Schiff et al., 1975); redecison therapy (Goulding & Goulding, 1979); body work designed to provide corrective experiences for the child (Cassius, 1980), self-reparenting approaches (James, 1981); child-development work (Levin, 1988); and rechilding (Clarkson & Fish, 1988); to name some. In addition, many transactional analysis practitioners recently have turned to modern psychoanalytic advances, and the transactional analysis literature and conferences related to transactional analysis have increasingly included such material. Clients whose problems originate in infancy do not respond to therapeutic operations such as explanation, confrontation, clarification, and interpretation. They tend to act rather than talk and to create circumstances in their lives that are dangerous to themselves or others, often prompting treatment. They tend to undo progress and are likely to leave therapy just when progress seems most promising. Those who display such characteristics usually fit within the narcissistic-borderline continuum (Adler, 1985) and are often diagnosed as schizophrenic, schizoid, analytically depressed, passive aggressive, psychopathic, impulse disordered, obsessive compulsive, eating disordered, or addictive--the spectrum of disorders originating in infancy. These clients, adamantly ego-syntonic with their Child's adaptations, are the ones we are concerned with in this article. Their psychiatric diagnoses are not considered here to represent classes of illnesses but rather methods of adaptations used by many of them to cope with a common, basic flaw stemming from early deprivation. In this article, a theory of the unwanted child syndrome is presented that shows how the aforementioned basic flaw brings about a particular splitting of the early Child ego state; how that splits leads to a situation in which the only relationship possible is one founded on hostility and dislike; and how the person's presenting symptoms serve to neutralize an intolerable internal experience that results from these developments. A novel treatment is then presented that corrects the structural distortions and brings to closure the original, early deprivations and their consequent developmental deficiencies. The Basic Flaw It is now universally recognized that early pathology develops from failure in the contact between the infant and the primary caregiver, usually the mother. Kohut (1971) wrote that, because of her own narcissistic fixations, a mother's self-absorption may lead her to project her moods and tensions onto the child or to respond inappropriately to his moods, resulting in the child's remaining "fixated on the whole early narcissistic milieu" (p. 66). Many of our clients in infancy experienced their caretakers as physically or psychologically unavailable. Here are some examples of disruptive attachment histories from my clients:
These clients feel unwanted and unloved and believe that they are unlovable. Echoing her early experience, one of these clients said:
In his famous study of infants temporarily separated from their mothers, Bowlby (1996,1973) found that if the mourning process and the environment are such that closure cannot be obtained, the infant will detach from its mother. It will first show distress at having lost the mother and will seek to have her back by any means. In time, the infant will become increasingly hopeless, withdrawn, and inactive and make no demands. It will become remote and apathetic toward the mother on her return. If loss persists, the infant will gradually become self-centered and replace an interest in people with a preoccupation with things such as sweets, food, or toys. It is reasonable to assume that detachment also results from unresolved emotional abandonment. This assumption finds reinforcement in Federn’s (1952) posthumously published paper on children’s responses to pain and frustration. He proposed that “repeated frustration in childhood can result in an impairment. . . When no repair is made--spontaneously, by helpful environment, or by psychoanalysis--coldness and dullness in all object relations are established for life” (italics added) (p.266). Structurally, the infant’s detachment represents an exclusion by the infant of its internalized mother (P1 in Figure 1). This blocking off of the experience of “mother” is of such far-reaching consequence to the child’s later development that therapy cannot be effective without first mending it. I call the exclusion of mother’s representation a basic flaw (not to be confused with Balint’s [1968] basic fault). 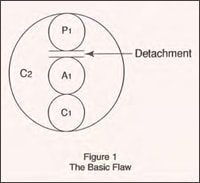
The Split
If the primary attachment is undisturbed, the growing toddler has enough of an internalized reliable early attachment figure to carry him through the initial exploratory ventures. Healthy and secure detachment can then lead to increased separation and individuation. But, lacking a reliable internalized mother, how can the detached toddler believe that he can venture out and survive? He solves this problem by splitting psychically, allowing one part of the psyche to take charge of and look after the other. The first part, here called the Tough Kid, “lifts itself up by its own bootstraps," its slogan being, "The hell with them all; I can do it myself." Magid and McKelvey (1987/1988) wrote, in regard to these unattached children, "It is as if a voice inside their heads is saying, 'I trusted you to be there and to take care of me, and you weren't. It hurts so much that I will not trust anyone, ever'" (p. 26). Bowlby (1977) described their quality as "compulsive self-reliance" adopted by the individual to seal his "destiny" of loneliness and to enable him to overcome his self-attributed unlovableness and low personal worth (p. 130). A client expresses this situation to the therapist thus: "Why should I accept you? I don't trust any adults. They are there to do what's good for them. Why will they care about me?" Serving as a substitute to the excluded, early internal mother image, the Tough Kid, made up to perform a parental function, may structurally be considered P1. But, as will be shown, there is more to the Tough Kid’s content and function. Once the split has materialized, the Tough Kid assumes the executive. It envelops and encapsulates the other, vulnerable part, called the Dependent Child (see functional diagram, Figure 2), and stands vigil to protect it from those who offer the greatest threat of abandonment--those with the potential for closeness or nurturing.
(It must be noted that this split is not the same as the splitting defense described in object relations theory. See the conclusion of this article for further discussion.) 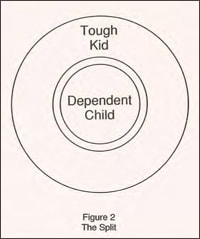
It is easy to detect the split early in treatment. For example, a teen-age client at her second session, after describing numerous abandonments and betrayals, says, “I don’t want to be dependent on anyone. I even hate to receive gifts. I don’t want to be helpless. I want to be in control and take care of myself.” When the therapist asks, “Is there a part of you that does want to be taken care of,” she replies with tears in her eyes, “Oh, yes, there is. It hasn’t been used for years. The only place I bring it out is in my poetry."
The Tough Kid mobilizes to cut off the Dependent Child from all contact that risks abandonment. But being only a split part of a young Child ego state, it is not equipped to substitute for the missing “good-enough” mother. As a consequence of the Tough Kid’s protection, the Dependent child is deprived of any yearned-for contact. It remains isolated and despondently lonely. This condition, discussed widely in the literature, is experienced by the client as an intolerable emptiness. Hartocollis (1977) described it as a state of chronic boredom, “a sense of longing for something (or someone) that is not merely absent, but nonexistent. . .something that leaves one empty or hungry. . .hopeful in a helpless way” (p. 497). The Tough Kid undertakes to protect the Dependent Child from these desolate feelings at all costs. It uses depression or other psychological symptoms and character traits to hide them from awareness, chemical addictions to anesthetize them, or psychosomatic illnesses or behavioral addictions to distract from these feelings. While the Dependent cChild harbors the feeling of desolate emptiness, it is the Tough Kid that retains the emotional memories of the early separation and protects itself, too, from the pain of these memories with additional methods (discussed in the treatment section of this article).
Revenge Behind the Child’s detachment lie his unexpressed rage and abandonment grief. Magid and McKelvey (1987,1988) wrote, “At the core of the unattached is a deep-seated rage. This rage is suppressed in their psyche. . . .Incomprehensible pain is forever locked in their souls because of the abandonment they felt as infants” (p. 26). The Tough Kid creates and maintains conflict with its mother, not only to find some outlet for this rage but also to fend her off and to defend itself from its own grief. It engages its mother in open or hidden behaviors of withholding or spite. According to Kohut (1972):
A client described his wish for revenge as follows:
Detached and unable to look after his own physical needs, the unwanted child must have some control over the mother’s attention. Lacking reliable attachment, he resorts to second best-contact through hostility. He cannot make the mother love but can surely make her hate him. Kirman (1989) wrote, “If we think about it, revenge is a way of holding onto the object while at the same time trying to get back at it. One has not let go of something if one is planning revenge against it” (p. 90).
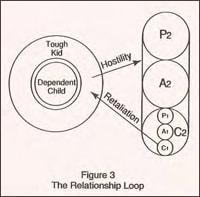
The child is not equipped to consider the consequences of his hostility, and these may turn out to be dreadful. The mother, narcissistically predisposed or unable to tolerate her own anxiety, responds to the child’s hostility with additional punishment or withdrawal (Kohut, 1971). In response, the child’s desire for revenge increases, leading to further escalation of the mother’s retaliatory responses. A self-reinforcing loop of mutual punishment, withdrawal, and dislike, open or disguised (Figure 3), ensues.
This feeling/behavior complex becomes the primary emotional contact available to the child and therefore most viscerally significant to him. A client eloquently described this situation when he said, “Hating is all I have left to keep going in the emptiness. Giving up hate is like dying, the last piece that connects to life.” Loneliness, punishment, and revenge become the essence of his attachment. Rejection, hostility, and hate are the feelings he seeks and strives for, and he assures their availability through his attachment behavior. Attachment Behavior
Attachment behavior has been defined as the class of behavioral systems aimed at maintaining contact with others, beginning with the mother. According to Bowlby (1996), the inborn programming of attachment behavior is continuously shaped and modified through experience, and the individual differences in experience lead to different patterns of attachment behavior. He wrote, “While especially evident during early childhood, attachment behavior is held to characterize human beings from cradle to grave” (Bowlby, 1977, p. 202). The evolving attachment behavior may be considered the early Child’s precursor to the script--the draft on which the script is elaborated--as the script (Berne, 1961) is “a complex set of transactions” that are “adaptations of infantile reactions and experiences” (p. 117). The presence of attachment behavior in the unwanted child seems to contradict the principle of exclusion. But the Tough Kid’s exclusion is one way. The Tough Kid maintains the privilege of excluding its mother, yet its survival requires that it have the mother maintain the tie. He accomplishes that task through the attachment behavior. The following excerpt captures the uncovering, in a session, of the detachment, the exclusion and revenge, and the resulting attachment behavior. The client--a professional woman of pleasant, though at the time vaguely irritating demeanor--had no close friends. Her marriage was conflict ridden. She was the mother of a young child, with whom she often struggled
These clients arrive at therapy with their attachment behavior at the ready. Soon, as the therapist begins to become significant to the Dependent Child, the Tough Kid will activate the attachment behavior through transactional activities. The client’s provocation may be open and frank but is more often hidden or disguised. He is a master at ferreting out others’ vulnerabilities (or gimmicks) and turning these vulnerabilities into mutually tormenting game payoffs. The more sophisticated players make the torment seem to be the victim’s fault.
In many cases, tormenting is the essence of the unwanted child’s racket or is masked behind a variety of roles, such as playing stupid, helpless, forgetful, confused, Woeful Wrongdoer, or Angry Righteous (Schiff et al., 1975). Revenge is served by any of the full range of transactional analysis’s pathological transactional activities. The Adult Under normal circumstances the Adult evolves in the second year of life to modulate and channel the Child’s striving and impulses according to present reality. Encountering its own emerging Adult, the Tough Kid assumes a stance toward it characterized by exclusion. After all, why should the Adult ego state be any different from other adults in the Tough Kid’s’ life? While excluding the Adult’s influence on it, the dominating Tough Kid may allow it to function in neutral, impersonal matters, but he makes sure to exclude it from the relationship field, both intrapsychic and interpersonal. While excluding the Adult, the Tough Kid nevertheless exploits it by using it as a conduit through which its attachment behavior flows. Thus, a client may seem fully rational while engaging the therapist in transactions characterized by blatant hostility (see Figure 4). 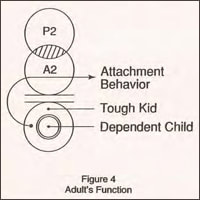
The Adult’s contamination by the Child is therefore of a special kind. It is characterized not by the usual overlap of the Child’s feelings, thoughts, and beliefs from earlier times, but by exclusion, exploitation, and domination of the Adult by the Tough Kid.
Lacking proper Adult functioning, the Tough Kid develops tricks and rules to deal with the demands of the complex world. But being only a developmentally arrested, splintered relic of early childhood, it is not equipped for proper Adult functioning. Many tasks that can be accomplished easily by adults are either impossible for the unwanted child or require extraordinary effort. 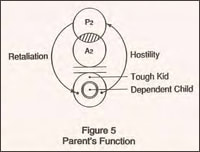
The Parent
No mention has been made so far of the Parent (P2) ego state because the split Child is fixated at an age earlier than the beginning of differentiation of the first-order Parent ego state. As the unwanted child grows, his Parent differentiates according to the historical unfolding of the growing child’s relationship with his caretakers. These relationships, characterized by the hostility-bound attachment behavior and dominated by the exclusion, define the later client’s Tough Kid intrapsychic relationship with its own Parent (see Figure 5). Treatment
The structural distortions described earlier are constructed by the child to allow, as best he can, for the treatment of his psychic survival that was presented by the abandonment. These structural rearrangements and their emotional and behavioral consequences become the life-restricting symptoms the client brings to therapy to resolve. But because the structural distortions are occasioned by the detachment at the original abandonment, the need to maintain these structural modifications disappears when the basic flaw is mended—the result is cure. The resolution of the basic flaw lies in the reversal of the emotional processes that led to the infant’s detachment. As mentioned earlier (Bowlby, 1973), detachment ensues when closure to the abandonment cannot be obtained. Because detachment is a defense against the intolerable pain of separation, the client must be helped to reenter that pain—with its feelings of rage, sadness, helplessness, aloneness, and hopelessness—and to arrive at a closure to his abandonment through the verbal expression of those feelings, that is, by fully mourning his early abandonment. When the basic flaw and the resulting split are mended, the client’s child will be able to, as it must, develop a trusting, dependent attachment with the therapist. This attachment, if found reliable, will allow the newly integrated Child to acquire the stable internal representation (P1) it needs to safely launch its quest for healthy separation and individuation. In essence, mending the basic flaw requires mourning, against which the client uses an array of defensive strategies. It is the Tough Kid who holds the emotional memories that are to be mourned as well as the defenses against them, and it is the Tough Kid who will mourn when these defenses are resolved. The attachment behavior provides the Tough Kid with a powerful defense against the feelings of grief by giving it an illusion of contact, thereby denying the reality of the separation. Grieving is also rendered impossible by the presence of first- and second-order exclusions. Like the infant during the original separation, the excluding Tough Kid is denied proper support for its mourning and is too young to mourn alone. The Tough Kid also defends itself by sharing in the defenses (described earlier) that it uses to protect the Dependent Child from the feelings of desolation. Of these defenses, Levin (1993) wrote:
Bern’s (1961) premise that patients have a functioning Adult that can be accessed and used therapeutically is a cornerstone of transactional analysis theory and practice. But when the Tough Kid dominates, it determines the nature and extent of the Adult’s functioning. At the beginning of treatment, the client’s Adult may be quite accessible; but as soon as the Dependent Child becomes interested in the therapist, the Tough Kid takes over. It excludes the Adult, neutralizes the therapist’s influence, and, exploiting the therapist’s vulnerabilities, enlists him in the attachment behavior. The client’s Adult, becoming merely a conduit through which the Tough Kid’s attachment behavior flows, is rendered useless as an ally to the therapist. In the absence of an uncontaminated, observing Adult, the client is egosyntonic with the Tough Kid, and the client’s cooperation in the therapeutic endeavor abates.
This is when treatment begins. The client’s attachment behavior should not be challenged but rather supported as a substitute for the missing therapeutic alliance. But if the attachment behavior is to be kept, then the usual transactional analysis treatment techniques are contraindicated. Games, rackets, and roles must be preserved to maintain the attachment behavior. Attempts to decontaminate the Adult will only stimulate the Tough Kid to increase its resistance. Redecision is premature in the absence of a sufficiently strong integrated Child. Explanations, interpretations, and confrontations will fall on the Tough Kid’s deaf ears. Positive stroking should be used selectively, and nurturing must be avoided, as it stimulates the Tough Kid’s opposition. The therapist must assume a neutral stance. Auxiliary Adult Now that the Tough Kid has arrived at its optimal relationship with the therapist and is poised to render further therapy useless, the therapist introduces a new therapeutic element for which the Tough Kid is completely unprepared. Bypassing the client’s existing Adult, the therapist calls on the client’s psychic resources to bring about a separate Adult entity. Under the therapist’s supervision, this entity, Trojan-horse fashion, will, for the duration of the treatment, help resolve the Tough Kid’s defenses and will eventually support the Tough Kid’s grieving work. The therapist disconnects himself from contact with the Child’s split parts and supervises the auxiliary Adult to provide the treatment in ways that the Tough Kid would never permit the therapist to attempt. To bring forth the auxiliary Adult, the therapist demonstrates the Child’s split to the client and then assigns one chair each to the Tough Kid, the Dependent Child, and the contaminated Adult (TK, DC, and Ao in Figure 6). A chair is then introduced for the new auxiliary Adult (Ax). The client is told that, when in that seat, he will, with the therapist’s help, be the one to work with the Child’s two parts. With this arrangement, the treatment shifts from the interpersonal to the intrapsychic. 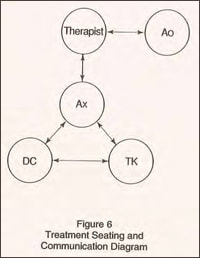
The client’s auxiliary Adult is given two tasks. First and foremost, it is to pay close attention to what is being said by either of the Child’s parts and every so often to repeat to that part what it had said. Second, it is to deliver to either part any interventions proposed by the therapist.
The auxiliary Adult has had no involvement in the client’s history. It meets the Child’s split parts for the first time and is not influenced by either Child part or by the Parent. Its tasks are reality bound, in the present. It is therefore wholly uncontaminated. Initially it contains little energy—just enough to fulfill its limited therapeutic functions under the therapist’s directions. As treatment advances, its allotment of psychic energy will increase, as will its function. The therapist, the auxiliary Adult, and the Dependent Child are thus aligned with a common goal: to treat the Tough Kid, who is, for the first time, outnumbered (the Parent is not involved in the process). The Process
Each therapy session begins and ends with the client in his contaminated Adult (Ao) seat. At the start of each session the client, in that seat, has ample opportunity to engage the therapist with his attachment behavior. The therapist must be able to tolerate this often painful contact. The therapist may also be accused of negligence, such as the client experienced at the hands of his early caretakers. Without retaliating or withdrawing, the therapist assumes, for therapeutic purpose, that all the accusations against him are correct (Spotnitz, 1993) and fully investigates each accusation with the client (e.g., “How am I being bad, cold, uncaring, etc.?”). At the first stage of treatment, the Tough Kid uses all the means at its disposal to reject the auxiliary Adult. Its actions are reminiscent of those of an antibody trying to isolate, engulf, and destroy a foreign object. To all the Tough Kid’s maneuvers, the auxiliary Adult responds simply by restating the Tough Kid’s statements. Here is an example:
The Tough Kid will accuse the auxiliary Adult, too, of the negligent behaviors the client experienced at the hands of his early caretakers. Through questions suggested by the therapist these accusations, too, will be investigated by the auxiliary Adult. The therapist will make sure to provide the auxiliary Adult with a steady supply of strokes for its performance to help fuel it with needed energy.
The Tough Kid will attempt to ensnare the auxiliary Adult in the attachment behavior. To these attempts the auxiliary Adult just keeps repeating what the Tough Kid has said. These repetitions have a profound effect. Eissler (1958) wrote that the effect of such repetitions may be equivalent to interpretations. Each successful restatement signifies to the Tough Kid that its assertions are understood and accepted, thus opening the way to the next, deeper level of expression. The auxiliary Adult, sharing a common body with both of the Child’s split parts, is able to restate at a level of understanding deeper than the therapist could ever achieve. In time, with the Tough Kid’s permission, the auxiliary Adult will make occasional contact with the Dependent Child and will continue the contact throughout the treatment. This contact, too, must be devoid of nurturing or positive stroking. As with the Tough Kid, the auxiliary Adult’s response will be limited to restatements.
Contact with the Dependent Child accentuates the tension between the opposing interests of the Child’s two parts. This tension provides the driving force to push the process forward to resolution. Contact with the Dependent Child should be neither too frequent nor too long. The proper treatment focuses on the Tough Kid, who is accustomed to being at the fore and will not object to attention that is directed at itself.
Given time, the passion in the Tough Kid’s hostility toward the auxiliary Adult subsides, and dependency wishes emerge. Whereas the Dependent Child’s yearnings are directed toward the therapist, the Tough Kid begins to express longings for its mother and experiences the despair over her absence:
With the loosening of the attachment behavior, and with the Tough Kid’s increasing acceptance of the auxiliary Adult, the Tough Kid’s defenses against grief give way, and depression and despair ensue. “ It’s a black pool now, not being wanted. Floating around. . .not even in any particular pain. In a black pool, around and around. . .Valley of the dead. To me it’s a horrible black.”
Given proper responsiveness by the auxiliary Adult through continuous paraphrasing, the depression is transformed into rage: “I hate you. I hate all of you. And you always have your reasons. It all sounds good. I feel hopeless and I hate you (cries)…I want to make you hurt for that. You made me hurt, and I want to hurt you back. I feel helpless with that.” As the rage is supported by the auxiliary Adult, it eventually subsides and is followed, finally, by mourning:
As the grieving progresses toward completion, these changes take place within each part of the ego state:
The auxiliary Adult's responses most often are on the mark. For example, to a quarrelsome utterance by the Tough Kid, the auxiliary Adult voluntarily responds,"I am watching over you. I feel calm. I am here and you can be as distant from me as you want." In response to the Tough Kid's expression of despair: "This is terrible stuff. You don't feel good with it. I feel sad for you." As grieving subsides, the auxiliary Adult, still uncontaminated, becomes sufficiently energized to take on full Adult function
The Tough Kid's exclusion of the auxiliary Adult at last collapses, leading to a full acceptance not only of the auxiliary Adult's presence but also its primacy.
Increasingly, the Tough Kid experiences the auxiliary Adult as caring, respectful, and affectionate, resulting in a crucial change in the Tough Kid's self-image and identity. Levin (1993) wrote, "The kind of self-love that makes possible a satisfactory and satisfying adult life is only possible if there are memory traces of being thought valuable, estimable, by somebody else: (p.84). As the Tough Kid incorporates these newly acquired feelings, its existential position shifts from the often-disguised "I'm not OK-You're not OK" to a frank "I'm OK-You're OK."
Eventually, the Tough Kid becomes indistinguishable from the Dependent Child, and the two are ready to merge. The merger should be negotiated between and initiated by the two split parts and not be an act of adapted compliance with perceived expectations from the therapist. The split is mended when the two finally merge.
The Contaminated Adult, no longer corrupted by the Tough Kid's manipulations, now becomes a vehicle for the expression of the integrated Child's Natural Child longings and responses instead, while still carrying Parent (P2) contaminations.
Outcomes
Afterward The client emerges from this treatment with his integrated Child developmentally at infancy and is prepared to revisit and complete subsequent unfinished developmental tasks. The therapist helps the client’s Child meet its developmental tasks by offering proper responses to presented developmental issues. Free of the unwanted child syndrome, the client welcomes and thrives on appropriate responses not only from the therapist and group members but also from others in his outside environment. Remaining treatment is associated with post-infancy problems. The Parent (P2) is reintroduced, and the usual transactional analysis strategies are used to decontaminate and neutralize its toxic influences. As the decontamination of the contaminated Adult progresses, uncontaminated early Child components dissolve into the newly integrated Child, and its decontaminated Adult portions merge with the uncontaminated Adult, resulting in the auxiliary Adult being exclusively in the executive. With that integration the client is cured, as the cause of his symptoms is permanently eradicated through fundamental changes in the structure and dynamics of his personality. Conclusion I call this modality treatment of the unwanted child rather than treatment of particular diagnoses. Use of this treatment should be determined by the internal structural characteristics of the client, not by his diagnosis. This is an intensive treatment, best provided at a frequency of one or more sessions a week. Group membership is recommended to provide the client with needed strokes and with opportunities to vent hostility, as well as a place in which he can safely generalize achievements obtained in individual sessions. This method should be considered an advanced technique to be attempted by experienced clinicians after it has been determined that the client indeed has the structural characteristics of the unwanted child and not a developmental fixation (such as in rapprochement) or a multiple-personality disorder. The split in the child described in this article should not be mistaken for the defense of splitting as referred to in object-relations theory. According to the object-relations model, mourning is not possible before the splitting defense is relinquished and the depressive position has been worked through (Levin, 1993, p. 261). In the case of the unwanted child, mourning is accomplished by one part of the split Child to make the mending of the split possible. Not all clients using the classic splitting defense have the structural characteristic described here. Conversely, not all who possess these structural characteristics necessarily use the splitting defense. I have used this treatment for about six years and have applied it at any given time to about a third of my clients. Its development is owed, with gratitude, to those clients who, despite frustrating, slow initial progress, nevertheless remained loyal to the mutual undertaking long enough to benefit from the results of the treatment they helped to develop. Aaron Lederer is an ITAA Certified Transactional Analyst (clinical) in private practice in Chatham, New Jersey. The author welcomes contact by clinicians whose interest is aroused by this article. Please send reprint requests to: Aaron Lederer, 244 Main Street, Chatham, New Jersey 07928, USA REFERENCES Adler, G. (1985). Borderline psychopathology and it treatment. New York: Jason Aronson. Balint, M. (1968). The basic fault: Therapeutic aspects of regression. London: Tavistock. Berne, E. (1961). Transactional analysis in psychotherapy: A systematic individual and social psychiatry. New York: Ballantine Books. Bowlby, J. (1969). Attachment and loss: Vol. 1. Attachment. New York: Basic Books. Bowlby, J. (1973). Attachment and loss: Vol. 2. Separation: Anxiety and anger. New York: Basic Books. Bowlby, J. (1977). The making and breaking of affectional bonds: II. Some principles of psychotherapy. British Journal of Psychiatry, 130, 421-43.1 Cassius, J. (1980). Horizons in bioenergetis: New dimensions in mind/body psychotherapy. Memphis, TN: Promethean Publications. Little, M.I. (1990). Psychotic anxieties and containment: A personal record of analysis with Winnicott. Northvale, NJ: Jason Aronson. Magid, K., & McKelvey, C.A. (1988). High risk: Children without conscience. New York: Bantam Books. (Original work published 1987). Rinsely, D. B. (1989). Developmental pathogenesis and treatment of borderline and narcissistic personalities. Northvale, NJ: Jason Aronson. Schiff, J. L., with Schiff, A. W.; Mellor, K.; Schiff, E.; Schiff, S.; Richman, D.; Fishman, J.; Woltz, L.; Fishman, C.; and Momb, D. (1975) Cathexis reader: Transactional analysis treatment of psychosis. New York: Harper & Row. Spotnitz, H. (1993). A theoretical outline of modern psychoanalysis. Unpublished manuscript. Steiner, C. M. (1974). Scripts people live: Transactional analysis of life scripts. New York: Grove Press. Download article in PDF format |